
You Have an Endometriosis Drug. Now How Do You Test It?

What is endometriosis?
I would argue that 2026 has been a pivotal year for endometriosis drug discovery. More public figures are sharing their experiences with the disease, and the biotech industry is investing more attention than ever into a condition that has been neglected for decades. Endometriosis affects approximately 10% of women of reproductive age and is characterized by painful lesions that can lead to chronic pelvic pain, infertility, and reduced quality of life. Yet despite its prevalence, relatively little investment has historically been made in understanding or treating the disease.
That is beginning to change. Pharmaceutical companies, from early-stage startups to large biopharma, are racing to develop new therapeutics. At the same time, agencies such as the NIH and ARPA-H have launched funding initiatives aimed at accelerating innovation in endometriosis research.
Despite this momentum, the underlying biology of endometriosis remains poorly understood. What initiates lesion formation? Why do some lesions progress while others remain stable? What drives disease flares? There is no single molecular "on/off" switch. Instead, endometriosis appears to arise from a complex interaction between hormone signaling, inflammation, fibrosis, immune dysfunction, and tissue remodeling.
What endometriosis drugs currently exist?
Fortunately, this section is relatively short. Every FDA-approved medication for endometriosis targets essentially the same biological pathway: gonadotropin-releasing hormone (GnRH). A quick look at the approved therapies shows little mechanistic diversity. GnRH agonists and antagonists suppress estrogen production, which reduces pain by limiting hormonal stimulation of endometriotic lesions. While effective for many patients, these therapies manage symptoms rather than treat the underlying disease biology.
Because estrogen suppression induces a temporary menopausal state, patients often experience hot flashes, bone density loss, mood changes, and other menopause-like side effects. Surgical removal of lesions is another common treatment option, but recurrence remains common, with approximately 20% of patients experiencing disease recurrence following surgery [Masferrer-Ferragutcasa, NPJ Women’s Health 2026].
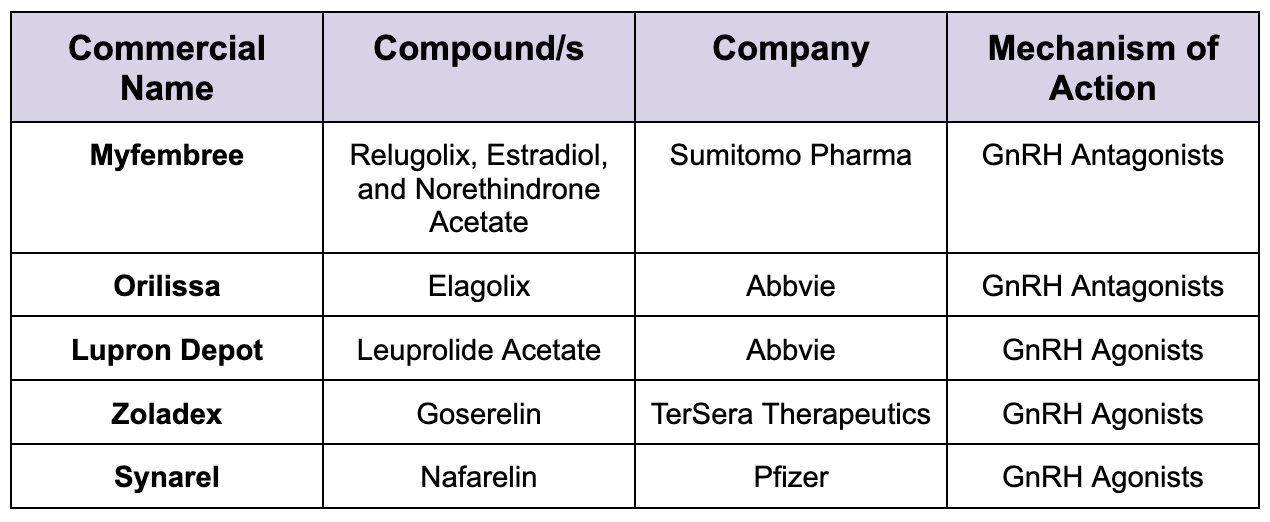
Table of current FDA approved drugs for endometriosis
From a commercial perspective, it is unlikely that new biotech companies will pursue another GnRH-based therapy. These drugs are well established, relatively inexpensive to manufacture, and the market is dominated by large pharmaceutical companies. Even newer entrants such as Myfembree have struggled to differentiate themselves because patients are seeking alternatives to therapies that rely on long-term hormonal suppression.
New compounds require new ways of testing
Fortunately, the pipeline is becoming much more diverse. Several companies are now advancing non-hormonal therapies that target the underlying biology of endometriosis rather than simply suppressing estrogen. Gesynta is evaluating vipoglanstat, an mPGES-1 inhibitor designed to reduce inflammatory prostaglandin production and lesion progression. Hope Medicine is developing a first-in-class monoclonal antibody targeting the prolactin receptor, which has shown encouraging Phase II pain reduction results. More recently, Gedeon Richter expanded its endometriosis pipeline through the acquisition of Celmatix and its portfolio of JNK inhibitors.
Although these compounds target very different biological pathways, they are largely evaluated using the same clinical endpoints: changes in dysmenorrhea and non-menstrual pelvic pain.
Patient-derived endometrial organoids faithfully recapitulate many of the inflammatory, hormonal, and fibrotic characteristics observed in endometriosis. Unlike conventional rodent models, they allow researchers to directly measure how experimental therapies influence lesion biology in human tissue. Rather than asking only, "Does this drug reduce pain?", researchers can also ask, "Does this therapy reduce fibrosis? Does it alter inflammatory signaling? Does it shrink lesion tissue or normalize disease-associated phenotypes?" The next generation of endometriosis therapeutics will likely be defined not only by new molecular targets, but also by better human models that allow researchers to understand which therapies truly modify disease before they ever enter the clinic.
At Opal Therapeutics, our goal is to make these human uterine models broadly accessible to pharmaceutical companies developing the next generation of endometriosis therapeutics. Instead of relying on rodent models that fail to capture the biology of menstruation and endometriosis, researchers can generate human-derived efficacy data directly from patient tissues. For decades, the lack of predictive human models has limited how many compounds could realistically be explored. We believe that bottleneck is finally beginning to disappear. As organoid technologies become standardized and scalable, they will enable researchers to rapidly evaluate new therapeutic approaches, opening the door to a new era of endometriosis drug discovery focused on human biology rather than animal surrogates.